IBCA sessions on building a claim service for people infected and never compensated
Purpose of the session
To hear directly from people who are infected and never compensated and their representatives, about how IBCA can design a fair, compassionate and accessible process for registration and making a claim.
Format
Three sessions were held between 6 and 8 October 2025. Each lasted around 90 minutes and brought together people who are infected and never compensated, along with individuals and representatives who support them.
We also held separate sessions with registered legal representatives and IBCA’s user consultants. These sessions built on earlier engagement about registration and prioritisation and focused on how people who are infected and never compensated will be able to make a claim for compensation.
Below, we’ve outlined the topics that were discussed and the views that were raised. You can see the slides that were shared in advance of the sessions.
Topic 1: Prioritising claims in private beta of those who have previously engaged with IBCA
The discussions opened with an explanation of what ‘private beta’ means: a small-scale test of the claims process with a small number of claims processed before it opens to everyone. IBCA said this phase would allow the organisation to identify and resolve issues early and make sure the full service works smoothly when launched. Participants were invited to share who they felt should be included first and how fairness should be defined.
Fairness and pace were central concerns across all sessions. Attendees asked IBCA to avoid designs that unintentionally exclude people who are exhausted, unwell, or retraumatised by the process, and to make choices that deliver payments quickly and fairly. Many attendees told us they already have complete evidence ready now. They asked IBCA to use this evidence in private beta to speed up decisions, rather than waiting for IBCA to collect it on their behalf. We also heard that taking part in roundtables and research has been retraumatising for many. People attended despite illness, caring responsibilities, and significant personal pressures.
There was agreement from the majority of attendees that end-of-life cases should come first with a sense that IBCA would be going “off-piste” should it deviate from this approach, but many questioned how that would be defined. Some asked if severe mental health issues or rapid decline in wellbeing would be recognised. “I am taking antidepressants and benzodiazepines to function while caring for a neurodivergent child. This process has added significant distress” one person said.
Others reflected on the emotional weight of living with infection for decades: “If I could have lived in ignorance, my mental health would have been a lot better.”
Several people urged IBCA to recognise moral as well as medical urgency. “Some of us have spent years fighting for recognition while watching others die waiting,” one said. “People need to be seen and recognised before it’s too late.” Another added, “I’ve been infected since the 1970s. There are no guarantees left for us.”
Attendees pressed for breadth within the first test cohort. They said that the initial claims in private beta should include a balance of infections, ages and backgrounds so that early learning reflects the whole community, not just those with liver disease. “This cannot be ten people paid in seven months and IBCA patting themselves on the back,” one said. “Make sure you listen to the first twenty [or more].”
Members of the Hepatitis B community spoke with frustration about historic exclusion. One participant explained that “There’s no cure. We’ve fallen down a priority rabbit hole.” Others said that earlier promises to consider Hepatitis B cases quickly had not yet been honoured: “We were rejected by Skipton, rejected by IBSS, appeals, judicial reviews — we shouldn’t be here still having to fight.”
Some participants argued that people with full evidence and/or those who had been supported by legal firms should be prioritised to help IBCA test the system effectively and quickly. “If the beta group doesn't have evidence it could hold everyone up,” one said. “If you go with people who already have everything ready, it’ll benefit everyone in the long run.” Others disagreed, warning that this approach could unfairly favour those who have been engaged with so far.
Several attendees challenged the suggestion that IBCA’s approach was guided only by the Inquiry’s recommendations. “You can’t just say there’s no consensus so you’re going with the Inquiry,” one said. “It doesn’t even mention private beta.” Another added, “Every time you say you’re following the recommendations, it sounds like a way to avoid deciding.”
Participants also raised the issue of interim payments. Many said that while IBCA cannot authorise them, it should press the government to act. “You have to tell the Cabinet Office the victims need an interim payment. Tell them directly,” one said, to widespread agreement. IBCA confirmed that all feedback for the Cabinet Office is passed to them.
IBCA confirmed that the first phase of private beta would include a smaller number of claims focusing on end-of-life cases and those with serious illness, while allowing discretion for exceptional vulnerability. It said that feedback from these sessions would also inform recommendations to the Executive Committee and Board.
Participants also told us they do not accept payments to affected people beginning before all living infected people have been compensated. They asked IBCA to reflect Sir Brian’s position and to seek community input before any sequencing decisions are made.
There was also discussion of a mixed private beta cohort that could combine people who are at the end of life or living with serious illness and people who had attended previous roundtables who already hold complete evidence without IBCA claim managers having to collect it.
Participants then spoke about the wider meaning of prioritisation. “How you decide who comes first tells us who you think matters most,” one said. Others reminded IBCA that transparency will build trust more than speed alone. “None of this feels fair right now,” a participant reflected, “but you can make it fairer if you listen and act.” IBCA confirmed that these sessions allowed it to listen, and act on views wherever possible (especially where a consensus was reached). IBCA also reiterated that Inquiry recommendations have outlined prioritisation.
Topic 2: Providing evidence of infection
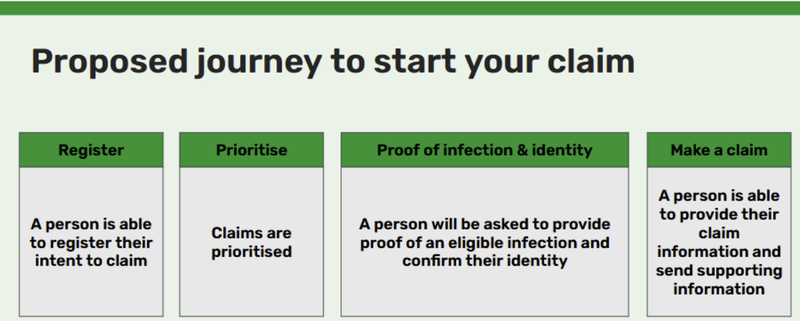
Part of the discussion focused on how people could show that they have an eligible infection. IBCA explained that after registration and identity verification, people would be asked for evidence to confirm eligibility. This stage is designed to protect the service from non-viable claims without creating unnecessary barriers.
From the outset, participants said the word “proof” was problematic: “The word ‘proof’ is unhelpful. Something like ‘indicative evidence’ would be better. ‘Proof’ will put people off even starting.” Another added, “The Hepatitis B community has never been believed. If you ask for ‘proof’, some will just shut down.”
Participants emphasised that tone and language will be crucial. “We’ve seen too much bureaucracy already. The word ‘proof’ feels like another barrier. It needs to sound supportive, not suspicious.”
There was concern about how people without documentation would be treated. “Say someone doesn’t have proof — where does a witness statement come in? Could that be enough?”
Several participants asked IBCA to clarify exactly what kind of infection evidence would be required. “You aren’t asking for proof of an eligible infection — it’s for proof of any infection.”
Another said, “You could have two options — they could provide information about the date of their infection if they have it, and the others could provide what they have with missing evidence.”
IBCA confirmed that the intention at this stage is only to establish that a person has an eligible infection, not to evidence when or how it was acquired. IBCA explained that proof of infection means showing medical confirmation of being diagnosed with hepatitis B, hepatitis C or HIV, and that questions about date or mechanism, if missing, did not need to be asked until later in the claims process.
Participants broadly welcomed that clarification, saying that “asking only for the infection itself feels achievable,” and that keeping the first step simple would “help people start without feeling interrogated.” However, a smaller number of participants raised concerns that some individuals may find it challenging to provide IBCA with medical confirmation of infections and that they would need to be supported at this stage.
People also reflected on the destruction of medical records and the harm it had caused. “The perpetrator destroyed what would prove an infection — IBCA must acknowledge that. People shouldn’t be punished for evidence that no longer exists.”
Participants shared frustration about earlier scheme rejections. “Don’t rely on rejection letters from IBSS. They didn’t always get it right. One in five were rejected in error.” Another said, “Doctors need training on the destruction of records. They haven’t been taught about the intricacies of this scandal.”
Others said the process must recognise that not everyone can interpret medical evidence. “Don’t presume people can read or understand their medical records. Ask, ‘Why do you believe you’re eligible?’ That’s a gentler and more humane question.”
Finally, participants also emphasised the importance of IBCA spelling out what support claimants could expect to receive at an early stage: “there will be lots of people ‘naive’ to the [claim] process and they will need signposting of the support that they will receive.”
The conversation closed with agreement that IBCA must make its expectations clear, keep the first evidence step simple and humane, and design guidance that builds trust rather than fear. “We can live with fair rules,” one participant said, “but we can’t live with being doubted again”.
Topic 3: Proving identity up front
This discussion focused on how IBCA will confirm a person’s identity before assigning them a claim manager. IBCA explained that this step is intended to prevent errors and protect the security and integrity of the service; its development has been influenced by feedback at previous engagement sessions.
Participants overwhelmingly said that they understood the need for identity checks, but views differed about how this should be done. “We’re all very used to having to prove our identity with a driver’s licence or passport.” Another said they were “less happy with Government Login – feels a bit Big Brotherish.”
Several people said they were comfortable providing standard documents but not photographs or digital uploads. “I wouldn’t expect not to have to give evidence of my identity,” one said, “but you want it to feel safe, not like surveillance.” Others felt that requiring both proof of infection and proof of identity before a claim manager is assigned was reasonable if handled simply.
Some questioned whether identity should come before or after prioritisation. “Could we not do identity once you know who is going forward?” one person asked, with others articulating that the proposed approach risked those without legitimate claims being prioritised ahead of those with legitimate ones. Others worried that an early verification stage could slow progress for those already ill.
Accessibility was another strong theme. “Three in ten people are going to struggle,” one said. “The older someone is, the more difficult it is going to be for these people.” Participants said that identity checks must not rely entirely on technology and that people should be able to complete them through familiar routes. “You want it to be simple and easy to understand,” one said.
A few attendees asked whether IBCA had already made decisions about how identity would be verified. “If you’ve already decided to use this,” one person said, “it makes this discussion meaningless.” Participants said that engagement should happen before decisions are finalised so that people feel genuinely listened to.
IBCA confirmed that One Login had been agreed as the digital option for confirming identity, but that non-digital routes would be available for those unable to use online verification. It added that these alternatives would ensure no one is excluded or delayed because they cannot access technology. The key question for discussion was when identity should be verified and how to support those who could not or did not want to use One Login.
The discussions all agreed that choice, flexibility and respect are essential. Participants said that people should feel secure, not monitored, and that verification should never become a barrier to recognition or payment.
Topic 4: Using GOV.UK One Login and supporting those who cannot use this
The final discussion further explored the proposed use of GOV.UK One Login to verify identity online and what alternatives should exist for people unable to use it. IBCA explained that One Login allows most people to confirm their identity digitally using a smartphone, email address and photo ID. Around seven in ten people are expected to be able to use it successfully (this is the broader success rate across Government, with an average of 3 in 10 not being able to verify themselves for various reasons), while supported routes would be available for others.
Participants shared mixed feelings. Many said that reliance on technology risks excluding those most in need of support. One explained that “three in ten people will struggle — the older you are, the harder it’ll be,” while another said that “it adds another burden to an already traumatised group.” Some described the idea of uploading sensitive documents (passport, driving licence, etc.) as uncomfortable or unsafe. They asked IBCA to guarantee that the process would be secure, optional and flexible.
One group was particularly concerned that the use of One Login was part of a wider government push around digital ID and expressed worry that IBCA had been instructed to use this platform by the government.
Attendees offered practical suggestions to make the system more inclusive. They proposed allowing claim managers to verify identity directly, letting people provide certified copies of documents by post, or using trusted intermediaries such as local councils, Citizens Advice or legal firms. Others suggested a process similar to passport countersigning, where someone who knows the person - such as a GP or Councillor - can confirm their identity.
Participants emphasised that anyone who chooses a manual route must not face delays or be disadvantaged. One said that “if people think choosing the safer option means waiting longer, they’ll see it as punishment.” There was broad agreement that equality of outcome should be guaranteed whatever route people take.
IBCA confirmed that One Login will be one option, but not the only one, and that supported and non-digital routes will be available. It will likely be the fastest and most secure route for many though, as it is digital (i.e. someone using it will receive an immediate confirmation, unlike postal options). IBCA thanked participants for their ideas, explaining that their feedback will shape how these options are designed and communicated.