IBCA sessions on registration and prioritisation with community groups
Purpose
The purpose was to gather views from community groups on IBCA's proposed approach to registration and prioritisation for compensation.
Format
There were seven community group sessions that took place virtually week commencing 4 August 2025 with representatives from community groups and individual campaigners. We have also included points raised during a session held with legal representatives, alongside the other feedback we received from community groups via email.
These sessions are about working with the infected blood community to ensure that IBCA's approach takes into account community views. This supplements other ways IBCA works with the community, including user research where users provide feedback on the design and improvement of the compensation claim service, and regular engagement sessions.
Below is an overview of the discussions that took place.
Introduction
IBCA provided an overview of the purpose of registration, including:
- Registration enables anyone intending to claim compensation to register their details with IBCA, as well as recording information that may help IBCA to prioritise claims based on the Infected Blood Inquiry's recommendations.
- It's not planned to check eligibility and identity at this stage, as identity verification (IDV) would come later, once a claim begins.
- Attendees were shown a draft version of what the registration form might look like. You can see the slides that were shared here.
Below we've outlined the main discussion points for the sessions, and views that were raised.
Participants advised that presenting documents in advance of the session would have allowed for more meaningful engagement and could have been shared with the wider community, to gather more feedback in advance of the online sessions.
IBCA note: a feedback form is provided on the website for further community views to be submitted.
Additional feedback emphasised that the Inquiry Chair’s Additional Report should be treated as the definitive basis for registration and prioritisation, with some concerns that the options presented by IBCA may diverge from those recommendations.
IBCA note: we have accepted all recommendations from the Infected Blood Inquiry’s Additional Report.
Discussion point 1
We have kept the scope of registration small to deliver it quicker and remove the identity verification barrier at this stage - do people agree with this approach?
The central theme of the discussions was a tension between speed and thoroughness. While there was broad agreement on the goal of getting compensation to people as quickly as possible, attendees felt that our proposed simplified registration process, which separates ID Verification (IDV) to happen when a claim begins, was the wrong approach. The majority of attendees said that a more robust, one-time process, even if it takes a bit longer initially, would be more effective in the long run. IBCA confirmed this would take longer to build, so a registration process would not be delivered in September if this approach was taken.
Our proposal to keep the registration process simple and not include IDV and evidence collection was based on a) the speed at which we could deliver registration for all community members and b) reducing the initial burden and time for those intending to claim. However, attendees believed that by not asking for IDV, IBCA could face a bottleneck at a later stage. Concerns were shared about fraudulent claims 'clogging the system', wasting time and resources. There was also a desire for IBCA processes to be as efficient as possible.
We asked whether people were comfortable if that would mean registration was more burdensome. A majority advised that genuine people claiming would be happy with this. A simple form without any verification would not provide reassurance or a sense of progress.
Suggestions from attendees
- Include a simple field for an EIBSS reference number if known.
- Provide a clear list of required documents during registration so people can begin gathering them.
- Allow claimants to upload supporting evidence with their registration to 'short circuit' the process later. It was noted that at present IBCA intends for this to be a later stage.
- The form should be designed to capture condition details, health status, and age to inform prioritisation within each group.
- The registration process should allow a person to register their intent to claim under multiple categories (i.e. estate claim and affected, unregistered infected and affected etc.)
- IBCA should work with IBSS and lawyers to register those whose information may be held.
- Capturing the type of claim people were planning to make could help IBCA plan and allocate resources and could allow some cohorts to be sped up.
- Need to ensure that the registration process is not confused with the starting of a claim and registering in and of itself is not the same as IBCA establishing a person wishing to claim is definitely eligible for compensation.
Further feedback stated that registration should be opened to everyone who may be eligible for compensation. It was suggested that the registration form should allow individuals to complete an application form, not just signal intent. Some participants also highlighted that the Recognised Legal Representatives (RLRs) already hold much relevant information and should play a central role in front-loading claims that could be brought straight to the declaration stage.
Claimants expressed concern that IBCA should have a dedicated team on data gathering to ensure this does not absorb Claim Manager resource.
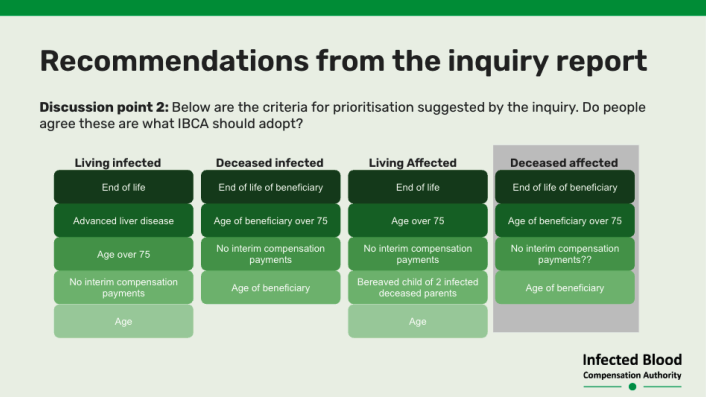
Discussion point 2
Below are the criteria for prioritisation suggested by the Inquiry - do people agree these are what IBCA should adopt?
While there was general agreement on some points, there was no overall consensus on prioritisation.
End-of-life and health-related criteria
While there was a clear majority opinion that prioritisation is necessary, there was no consensus on the specific criteria. Some supported the Inquiry's proposals while others felt they were not adequate.
There was significant conflict and concern over the issue of prioritisation, particularly concerning those impacted by the September 1991 cut-off date.
There was a strong consensus that individuals with a terminal diagnosis or those at the end of life should continue to be the top priority. Attendees challenged the narrow 'end-of-life' category, arguing that it should be expanded to include the frail, elderly, or those with age-related illnesses.
The Inquiry's category of 'advanced liver disease' was seen as too narrow. Stakeholders advised a more holistic view of health, suggesting that other serious conditions like liver cancer, psychological issues, PTSD, dementia, Alzheimer's, thyroid disease, and conditions resulting from Interferon treatment should also be considered.
The question of how to prioritise those who are claiming on behalf of someone who was infected and is now deceased, was also raised as a complex and potentially unworkable issue.
A specific suggestion regarding deceased infected claims was to prioritise those beneficiaries at the end of their lives and then IBCA should start processing the claims from the date of death (earliest death first) - that would be a method that would capture earlier those who died too early to be eligible for any previous financial support and the parents of those who lost children.
Additional feedback also suggested that prioritising based on conditions such as "advanced liver disease", "liver cancer" and "conditions resulting from Interferon treatment" would unintentionally exclude people who are in poor health due to suffering from HIV related conditions.
Feedback was also received that infection type alone should be a standalone category for consideration in prioritisation.
A suggestion would be to add criteria for those living with the consequences of HIV or AIDS and could mirror conditions that are compensated in the supplementary route to ensure a more holistic and inclusive approach.
Age
There was significant disagreement regarding the use of age as a prioritisation criteria. The suggestion to prioritise those over 75 was seen by some as being unfair to younger individuals who have suffered for a lifetime and some felt, for this reason, that date of diagnosis or infection should be considered. Others felt that age was a key factor, particularly for bereaved parents who are elderly and sick. A specific suggestion was to prioritise those aged 70 or over, or even 65.
It could not be agreed whether age should be a prioritisation factor. The conflict stemmed from some feeling that a focus on age could unfairly benefit those who have already received some form of compensation while overlooking the long-term suffering of others.
Fairness, justice, and long-term impact
There was a consensus that the proposed criteria lack a sense of justice and fail to acknowledge the long-term impact on people's lives.
Attendees felt that the approach suggested by the Inquiry ignores those who have lived with the knowledge of their infection for decades, as well as children who lost parents at a young age and bereaved parents. There was a feeling that people with a recent impact are being prioritised over those who have had a lifelong impact, which is seen as an injustice.
Suggestions from attendees
- Prioritise by date of infection or diagnosis to reflect the long-term impact on a person's life.
- Prioritisation criteria should be broader than just a terminal diagnosis and should be sensitive to age-related illnesses.
- IBCA should address the previous issues cut-off dates and segregation between registered and unregistered individuals by prioritising the unregistered infected.
- The system should not be set up in a way that separates family members; instead, it should deal with a claim and the 'immediate web of people attached to that person's estate at the same time.'
- Understanding the reasons behind a lack of interim payment is crucial for ensuring fairness and addressing historical injustices.
Concerns
There was a shared concern that the process could be easily exploited, particularly with self-reporting criteria.
While many agreed that end-of-life should be a priority, there was concern that relying on self-reporting without a burden of proof could lead to fraud and unfairly push others down the queue.
Feedback also raised concerns that the inclusion of interim payment status in prioritisation risked misinterpreting the Inquiry's intent. Interim payments were intended only as a reason to ensure those who had not yet received any compensation were prioritised, not as grounds to de-prioritise those who had received them.
Additional feedback noted that some affected individuals - such as widows, bereaved parents, or divorced partners who are not estate beneficiaries - risk being excluded if prioritisation is tied too closely to estate status. These groups, often elderly and vulnerable, should still be prioritised, we heard.
Suggestions from attendees
- The date the registration form was submitted could be a factor in prioritising claims where other criteria are exactly the same.
- A dedicated team should be created to process claims from unregistered individuals to prevent a bottleneck that could push back other claims.
- Participants expressed a desire to have a prioritisation working group as they felt it needs more work than the Inquiry recommendations.
- Other feedback was to keep it as simple as possible as some people will struggle even with the most basic form.
- Suggestion that legal support offer might be usefully extended to registration to help those individuals.
Discussion point 3
We anticipate there will be occasions when we need to (or could choose to) start claims which are lower on prioritisation criteria but are linked to a claim being processed. Our intention (once the service is open to all types of claims) is to deal with all claims an individual has at the same time - so if someone has an infected and affected claim and one is started we would do both at the same time. Does everyone agree this is the right approach?
The discussion on linking claims within a family unit revealed strong and almost unanimous initial support, but as the practical implications were explored, significant conflicts and complex nuances emerged. While most agreed with the concept of a 'family unit' approach, there was no overall consensus on how to implement it without creating new forms of perceived unfairness.
There was strong, near-unanimous agreement with the principle of dealing with all claims from an individual or family at the same time. Attendees felt this would be more compassionate and efficient by minimising trauma from repeated contact and evidence requests, simplifying claim work, and preventing perceived unfairness where one family member's claim progresses while others do not. The idea of 'batching families' was seen as an efficient way to streamline the process. However, participants noted the issue of this potentially meaning younger and healthier people would be prioritised over older people.
There was general agreement that, wherever operationally possible, the same claim manager should process all claims for living infected, affected and deceased infected members of the same family and this would be the most efficient way of paying people more quickly.
While the principle was supported, the practical application raised concerns. A key point of contention was whether a lower-priority claim (e.g., an affected child) should be fast-tracked simply because it is linked to a higher-priority claim (e.g., an infected parent).
This led to a split view: some saw it as a logical, efficient approach, while others felt it would introduce a new type of unfairness.
There was a broad, underlying agreement that prioritisation is necessary, but that it must be done in a way that feels just and fair.
Some attendees felt that no affected person should be paid before a living infected person. This was challenged by others who said that linking families would get money to people more quickly, even if that meant an affected person received payment before an infected person.
The 'over 75' prioritisation was again raised as a point of contention, with concerns that linking claims could result in younger, healthy family members being prioritised over older, sicker individuals who are not part of a linked claim.
No majority opinion. There was no consensus on the prioritisation of linked claims (e.g., infected first, or a family unit first).
Concerns
Attendees were united in their view that IBCA's systems should be designed to be as efficient as possible.
Stakeholders felt that IBCA has not used existing information effectively. They suggested that IBCA should have already been capturing family member details through existing schemes (e.g., EIBSS). There was also concern that a lack of proper ID verification at the initial stage could be a missed opportunity to link claims and would lead to future administrative burdens. The experience of processing claims from the registered, living infected on IBSS is that a lot of the information required to make an accurate calculation has not been readily available at the beginning of the claim process.
Suggestions from attendees
- Use IBSS numbers or other existing data to link family claims and make the process more efficient.
- An individual's consent must be obtained before their personal data is used for a linked claim, especially in cases involving abusive ex-partners.
- The registration process should be designed to capture family member details.
- The number of claims managers should be scaled up to deal with a larger volume of claims simultaneously, which would mitigate the need to 'ration resources' and avoid complex prioritisation.
They requested more time in future to review documents and the ability to convert them into surveys for their members to comment on. To note that we have published these full notes on our website so that community members can let us know if any issues have not been raised already.
The broad consensus was that affected should follow infected claims (i.e. that IBCA should only open to affected claims once the infected claims have been handled rather than affected claim prioritisation influencing infected claim prioritisation). General agreement was that this is difficult and there will be a range of views.
Re prioritisation between cohorts, everyone broadly agreed that it would be odd for an affected claimant to be prioritised before an infected claimant e.g. on the grounds of age.
- Discussion as to whether it would be administratively easier to deal with groups by infection (so start with the infected person and then deal with all associated affected claims immediately thereafter). This has the advantage of dealing with the whole family at once (infected people are often just as concerned about ensuring their family has been provided for as they are for themselves).
- But this may only be a workable solution in harmonious family scenarios - there will be a challenge in dealing with affected people where there are disputes with the infected person and/or other family members.
- There are also some significant data protection challenges if an affected claim is determined before the underlying infected claim - IBCA would have to obtain medical records of the infected person to establish the affected claim - this will be controversial in difficult family scenarios. This problem doesn't exist to the same extent if IBCA determines all infected claims first - regulations relieve evidential burden if IBCA is already satisfied as to eligibility of underlying infected claim (as per reg 66(2)).
- Some major challenges lie ahead as regards estates - IBCA won't have the information we need for prioritisation readily available and will face broader probate challenges as well as risk of fraud.
Additional suggestions included creating a simple disputes mechanism, so if a person feels they have not been prioritised correctly, they can contact IBCA to check the data and registration.
Discussion point 4
Should we tell people where they are in the prioritised list? Since priorities can change, their position won't reliably predict start dates and may move. If we do share positions, how do we explain this clearly and sensitively?
Note: One group didn't discuss this point due to running out of time.
There was a general consensus that IBCA should share information about prioritisation status, with the caveat that communication must be clear and carefully managed. Community members wanted reassurance, especially if they are concerned about the length of time they had available to claim due to illness, and felt that sharing an estimated timeline, even if approximate, would be seen as honest and helpful. The benefits of providing clarity were viewed as outweighing the risks of disappointment or confusion.
However, while people want clarity, they do not want to see a specific number that could change. One attendee said, "I want timescale and clarity but don't want a number. It causes more stress and trauma." There was a strong feeling that providing a specific number would lead to anxiety, disappointment, and a sense of being 'a number.'
There was strong agreement that the community is highly traumatised, and any communication must be managed with extreme care. Participants shared a deep concern that telling someone their position could destroy their mental health, create false hope, and lead to retraumatisation if they see themselves 'fall back in the list.'
Suggestions from attendees
- Offer an opt-in during registration, asking people if they want to know.
- Publish aggregated cohort data (e.g., how many people from each group have come forward to register) instead of individual ranks.
- Provide an estimate of when a claim will be opened, expressed in weeks, months, or quarters, rather than a position number.
- Send a simple acknowledgment to confirm a registration form has been received. This simple step was seen as a meaningful way to provide reassurance without creating false expectations.
- It was strongly recommended that IBCA consults with psychological experts on how to manage expectations without causing additional stress.
- Everyone was generally against the idea of letting people know their 'number' in the 'queue' - dynamic prioritisation in itself would likely be well received.
- General feeling that everybody is desperate to register - and that the most likely outcome is for the vast majority of people to register upfront and there would be little influx after that.
A strong alternative view emerged that IBCA should focus on providing timelines and clear communication about the process, rather than a numbered list.
Discussion point 5
Are there any other factors we should consider when prioritising? Should we consider safeguarding as an additional priority area? Length of registration time (e.g. a person registering tomorrow will be prioritised accordingly and could be the next person to start their claim)?
Note: Not all groups discussed the following point due to time constraints.
The discussion on additional prioritisation factors highlighted a strong consensus on the need for flexibility and a compassionate approach beyond the initial criteria. While there was broad agreement on the importance of safeguarding, views were mixed on other factors, and no single majority opinion emerged on a comprehensive list. The feedback centered on identifying and protecting the most vulnerable claimants.
There was broad agreement that safeguarding is a critical and important factor that should be considered when prioritising claims. Participants raised specific concerns about substance misuse, drug and alcohol dependency, and individuals at risk of coercion or financial abuse, including from those close to them. A request was made for IBCA to provide guidance on how safeguarding will be handled, including processes for fraud prevention, risk assessment, and ensuring claimants are protected.
Suggestions from attendees
- Include homelessness as a prioritisation factor, with a request for a 'no fixed abode' option in the registration form.
- Ensure there is a mechanism for identifying and responding to exceptional cases, as long as the rationale is clear and defensible.
Views were mixed on whether to prioritise based on financial hardship, such as debt, poverty, or job loss. Some felt it was important to support vulnerable people, while others felt it could divert from the compensation's true purpose, which is to address harm caused by the infection, not financial need.
There was a general appetite for flexibility where justified. The community agreed that a 'common sense approach' is needed. One participant felt that ranking severity of illness was unworkable, but participants felt that IBCA should use its own judgment while being open with the community about how it was doing so.
Suggestions from attendees
- It was agreed that there should be a mechanism for identifying and responding to exceptional cases.
- Decisions should be based on a defensible rationale.
- The overall takeaway was that there should be flexibility in the system, provided the rationale is clear.
Some additional feedback said that undue emphasis on rare cases of family disputes, coercion, or individual risk factors such as homelessness or substance misuse could risk overshadowing the majority experience.
Discussion point 6
If we discover information on which we based prioritisation is incorrect while processing a claim, should we continue processing the claim or stop processing the claim, and correctly prioritise them?
Note: Not all groups discussed the following point due to time constraints.
The discussion on how to handle incorrect prioritisation information revealed a strong consensus that the approach should be fair, compassionate, and based on the nature of the error, rather than a one-size-fits-all rule. The central theme was the need to differentiate between an administrative mistake, a genuine human error, and deliberate misrepresentation.
There was a strong consensus that the course of action should depend on who was at fault for the error. Participants agreed that if the error was a result of an IBCA administrative mistake, the claim should continue to be processed without penalising the person. Conversely, if the error was a result of misleading or deliberately false information, the case may need to be reassessed.
The overarching goal should be to uphold fairness while avoiding unnecessary delays or retraumatising people. Attendees stressed the importance of distinguishing between dishonesty and genuine mistakes, and that honest errors should not automatically disqualify people or delay their claims.
Suggestions from attendees
- Create a clear framework that differentiates between IBCA administrative error, unintentional claimant omission, and deliberate misrepresentation.
- Ensure that a simple omission or honest mistake is handled with a flexible and compassionate approach, without penalty.
- Transparency and upfront clarity about evidence requirements from the beginning could minimise these errors.
Additional feedback noted that while it is important to distinguish between genuine mistakes and fraud, there was concern that undue emphasis on this issue risks distressing the wider community.
Additional feedback not tied to one discussion point
There was a request that IBCA produce dedicated information for widows and bereaved partners, setting out all the information that will be required for a deceased infected claim to reduce confusion and anxiety.
A suggestion that IBCA could ask infected individuals who had gone through the claim process, or executors for deceased infected people, for a list of linked individuals and use this information to register people proactively.